
Medical information notice
This guide is educational and does not replace professional medical advice. A licensed clinician should evaluate your history, labs, and medications before starting or changing treatment.
Long-term diabetes care requires a strategy — not just lower numbers
Type 2 diabetes is not a short-term condition. It is a chronic, progressive cardiometabolic disease that affects more than blood sugar alone. Over time, diabetes can influence cardiovascular risk, kidney function, metabolic health, and overall quality of life. Effective management therefore requires more than “lowering glucose.” It requires a plan that adapts as the disease evolves.
This guide explains how clinicians approach long-term diabetes and cardiometabolic care, where medications like Metformin, Mounjaro, and Trulicity fit, and why combination therapy is sometimes the most appropriate option.
Helpful next steps: Start consultation • Diabetes meds • More resources.
Understanding Type 2 diabetes as a cardiometabolic condition
Modern diabetes care does not treat Type 2 diabetes as an isolated blood-sugar problem. Instead, it is understood as part of a broader cardiometabolic picture. Many people with Type 2 diabetes also have insulin resistance, excess visceral fat, abnormal cholesterol levels, hypertension, and chronic low-grade inflammation.
These factors often appear together and increase the risk of heart disease, stroke, and kidney complications. That’s why contemporary diabetes plans increasingly focus on outcomes beyond glucose — including cardiovascular and kidney protection — while still pursuing safe, personalized glucose targets.
What clinicians track over time
- A1C trends and daily glucose patterns
- Blood pressure and lipid profile
- Weight and waist/visceral adiposity signals
- Kidney function markers (as appropriate)
Why it matters
Better long-term outcomes come from treating the whole metabolic system — not just fasting glucose.
Metformin: the foundation of long-term diabetes therapy
For decades, Metformin has remained a cornerstone of Type 2 diabetes treatment. It is commonly used as first-line therapy unless it is contraindicated or not tolerated. Clinicians rely on Metformin because it targets core disease physiology and has a long safety record.
How Metformin works
Metformin primarily improves insulin sensitivity and reduces excess glucose production in the liver. Unlike medications that push the pancreas to release insulin, Metformin does not directly stimulate insulin secretion — which is why it generally carries a low risk of hypoglycemia when used alone.
Why Metformin remains first-line for many patients
- Extensive clinical use and familiarity
- Strong safety profile for appropriate candidates
- Low cost and broad accessibility
- Useful base therapy that can be combined with other medications when needed
For many patients, Metformin forms the backbone of long-term care — particularly earlier in the disease course. But Type 2 diabetes is progressive, so treatment often evolves over time.
When Metformin alone is not enough
Metformin can be highly effective, but it may not provide adequate control indefinitely for every patient. Clinicians regularly reassess the plan when A1C goals aren’t met, cardiometabolic risk increases, or new health priorities emerge.
Important reframing
Needing additional medication is not “failure.” It often reflects the natural progression of Type 2 diabetes and a proactive approach to preventing complications.
At this stage, clinicians may consider adding medications that address multiple pathways — supporting glucose regulation while also improving weight and/or cardiometabolic risk where appropriate.
GLP-1 therapies: where Mounjaro and Trulicity fit in diabetes care
GLP-1–based therapies were developed for glucose control through multiple complementary mechanisms. They can be considered when individualized clinical goals include improved glycemic control, cardiometabolic risk management, and—when appropriate—weight reduction.
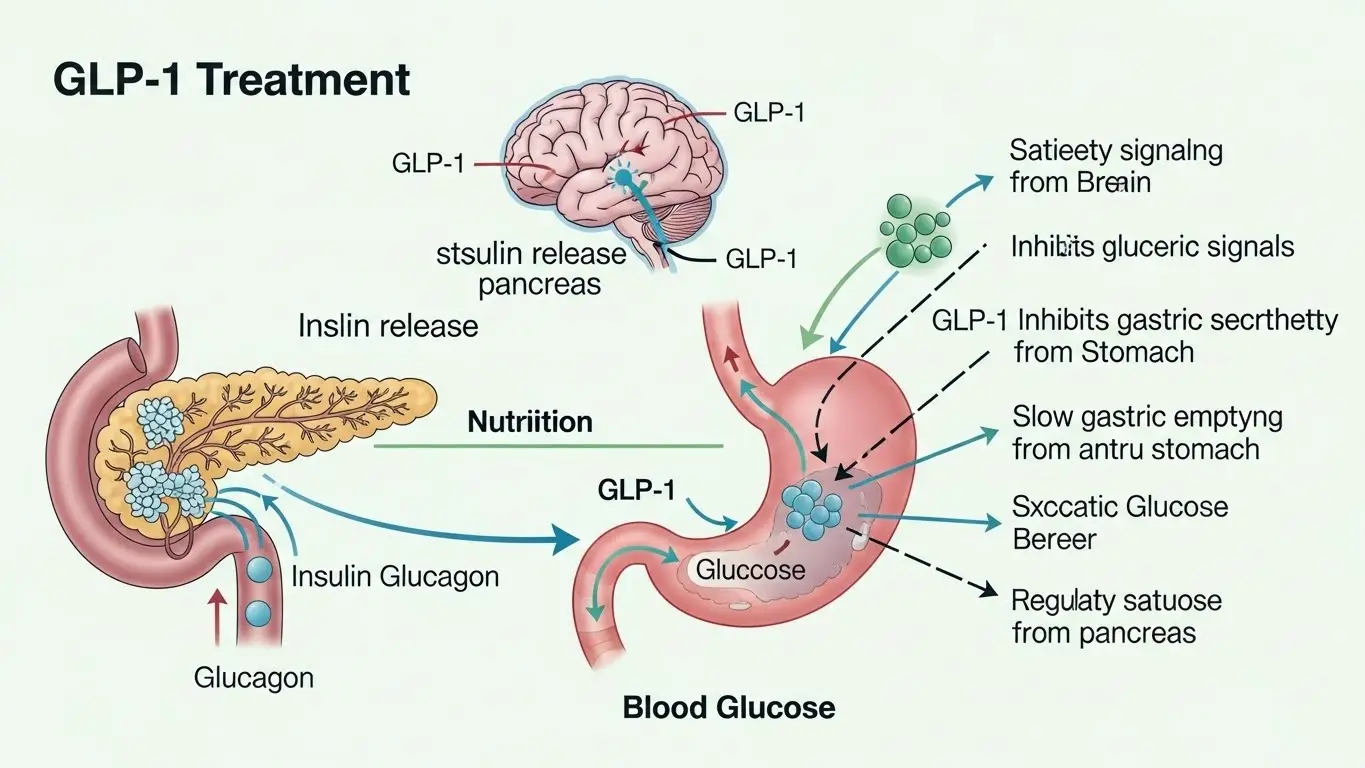
How GLP-1 therapies support glucose control
- Enhance insulin secretion when glucose is elevated
- Reduce inappropriate glucagon release
- Slow gastric emptying
- Increase satiety and reduce appetite signals
Because their action is glucose-dependent, hypoglycemia risk is generally low when not combined with medications that can cause low blood sugar. A clinician evaluates the full regimen.
Benefits beyond glucose for appropriate candidates
In addition to glycemic improvement, many patients experience weight reduction and improvements in cardiometabolic markers. This is one reason GLP-1 therapies are increasingly used as part of comprehensive diabetes strategies—not just for weight management.
Mounjaro vs Trulicity: how clinicians think about the choice
While both therapies act on incretin pathways, they are not identical. Clinicians don’t choose based on popularity. They consider the patient profile and treatment objectives.
Glycemic goals
How far current values are from target and how quickly control is needed safely.
Tolerability
Side effects, prior medication history, and ability to follow a titration plan.
Risk profile
Cardiovascular risk, kidney health considerations, and other coexisting conditions.
The “best” medication is the one that is appropriate, tolerable, and sustainable for a specific person—not a one-size-fits-all pick.
When clinicians combine diabetes medications
Combination therapy is common in long-term diabetes management because Type 2 diabetes affects multiple biological pathways. Using two medications can sometimes achieve better control at lower doses, with improved overall balance between effectiveness and tolerability.
Why combination therapy may be appropriate
- Single-agent control is insufficient
- Cardiometabolic risk reduction is a priority
- Weight management supports overall health goals
- Benefits outweigh risks for the individual patient
Key point
Adding a medication is not “giving up.” It can be a proactive, evidence-based move to reduce complications and keep therapy sustainable.
Monitoring, dosing adjustments, and follow-up over time
Long-term diabetes care is dynamic. Clinicians monitor results, side effects, and health markers to ensure treatment remains appropriate. Dosing may be adjusted, titrated gradually, or changed based on response and tolerability.

Patients should report symptoms early and ask questions. Follow-up helps clinicians refine the plan and decide if dose adjustments or changes are needed.
Urgent symptoms
If you experience severe symptoms or signs of a medical emergency, seek urgent medical attention immediately.
Frequently asked questions
Is Metformin still the first-line treatment for Type 2 diabetes?
Metformin is commonly used as first-line therapy for many patients due to its long clinical history, safety profile, and effectiveness in improving insulin sensitivity, unless it is contraindicated or not tolerated.
When are medications like Mounjaro or Trulicity added to treatment?
They may be added when glucose targets are not met on existing therapy, when cardiometabolic risk reduction is clinically appropriate, or when weight management supports overall health goals.
Can Metformin be combined with GLP-1 therapies?
Yes. Clinicians often use combination therapy—such as Metformin plus a GLP-1–based medication—when it is medically appropriate and the benefits outweigh potential risks for a specific patient.
Are GLP-1 medications only for weight loss?
No. GLP-1–based medications were developed for glucose control and cardiometabolic outcomes. Weight effects can be a secondary benefit for some patients.
How do clinicians decide on long-term diabetes treatment?
Clinicians consider glucose trends (including A1C), cardiovascular risk, kidney health, weight, tolerability, lifestyle factors, and patient goals—then adjust therapy over time as needs change.